




Context and Research Questions
Stunting is characterized by a height, weight, or body mass index below expected values, or by a variation in the height-to-weight ratio exceeding two percentiles on age- and sex-specific growth charts in a child whose growth had previously been normal (Tang et al., 2021). It results from prolonged exposure to inadequate nutrition, diseases and infections, and a lack of psychosocial stimulation (World Health Organization [WHO], 2017). This condition, which mainly appears before the age of two, has long-term effects on cognitive and physical development, academic achievement, and health in adulthood (Walker et al., 2007), hence the growing interest shown by international health and development strategies in this issue (UNICEF et al., 2023).
Since 2011, Senegal has been contributing to the Scaling Up Nutrition (SUN) initiative by strengthening its institutional structures and programs (Offosse N’Gbesso, 2018). The National Nutrition Development Policy (PNDN), led by the National Council for Nutrition Development (CNDN), has expanded access to nutrition services (Government of Senegal, 2015). It does so through community-based initiatives aimed at improving maternal and child health, hygiene, and access to healthy food and healthcare. It is implemented through the Multisectoral Nutrition Strategic Plan (Plan Stratégique Multisectoriel de la Nutrition – PSMN), which promotes an integrated approach and encourages the involvement of other stakeholders in the nutrition sector (Government of Senegal, 2018). Furthermore, within the framework of the Plan for Emerging Senegal (Plan Sénégal Emergent – PSE), investing in the fight against malnutrition is considered an effective strategy for strengthening social protection, community resilience, and stimulating economic growth (Government of Senegal, 2019).
The Nutrition Enhancement Program (PRN), under the leadership of the CNDN, aims to fight chronic malnutrition among children under five by mobilizing community, ministerial, and technical stakeholders. The PRN has strengthened governance in the field of nutrition and improved access to nutrition services for vulnerable populations. Since 2019, the Investment in the Early Years for Human Development Project in Senegal (Projet d’investissement dans les premières années pour le développement humain au Sénégal – PIPADHS), in partnership with the World Bank, has continued this momentum by investing in integrated interventions in nutrition, early childhood development, and education, mainly in rural and peri-urban areas, while also promoting women’s empowerment.
These efforts have led to a reduction in stunting, which decreased from 26.7% in 2011 to 17.9% in 2019, a rate below the African average (30.7%). However, in 2023, the prevalence reached 18%, including 4% severe forms (Figure 1), indicating a concerning stagnation.
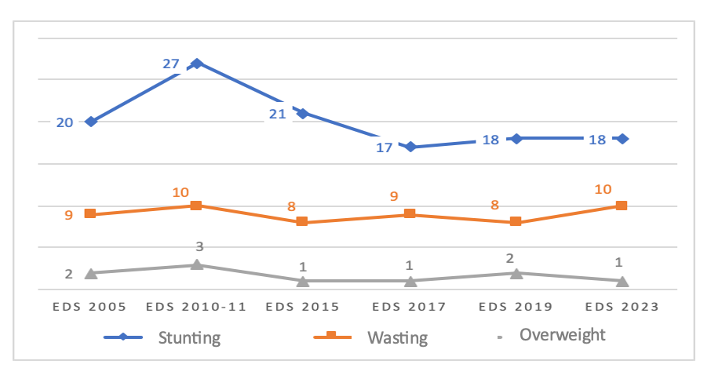
DHS data (2005–2023): a gradual decline in stunting from 2010–2011, relatively stable levels of wasting, and a persistently low prevalence of overweight among children.
Persistent regional inequalities can be observed. Certain regions, such as Saint-Louis, Matam, Kaffrine, and Kédougou, record stunting rates between 20% and 29%, reflecting their historical vulnerability to food insecurity (Pouye & Fall, 2023). In 2017, the southern and central regions of Senegal were the most affected by this condition, particularly in rural areas (20%) compared to 12% in urban areas (EDS-C, 2017).
According to UNICEF (1990), chronic malnutrition results from immediate factors, such as insufficient food intake or illness, as well as underlying factors related to food security, caregiving practices, and the health environment. It is also influenced by fundamental factors related to the social, economic, and political context, as well as available institutional and financial resources. Although this model highlights the interaction among these factors of malnutrition, it does not systematically take into account the influence of social norms, informal structures, and local power relations. In the context of arid regions of Africa, Young (2020) proposes a framework specifically for analyzing acute malnutrition, which retains the analysis of immediate and underlying causes while reconfiguring fundamental causes around three dimensions: the environment and seasonal variability, institutional systems, and people’s livelihoods. This approach emphasizes an integrated and contextual analysis and advocates for the active involvement of communities in designing more sustainable and contextually appropriate interventions.
Childhood stunting results from a complex interplay of factors, including immediate causes (inadequate food intake, disease), underlying causes (access to healthcare, water, and sanitation), and structural causes related to poverty and inequality (WHO, 2013). The prevention of stunting relies on adequate nutritional intake, psychosocial stimulation, nutrition and health interventions, as well as favorable environmental conditions. In the Senegalese context, Brar et al. (2020) developed a modified version of the stunting model by identifying distal determinants (climatic and economic shocks), intermediate determinants (access to healthcare, water, and food), and proximal determinants (maternal health, anemia, infectious diseases, age, and sex), enabling a more contextualized analysis of this disorder.
These approaches tend to reduce the impact of social and cultural norms, informal systems, and gender relations on nutritional status (Saidu & Danielson, 2024). In Senegal, local and community knowledge systems offer social interpretations of growth, as well as norms related to pregnancy, breastfeeding, and feeding practices (Moreno et al., 2023). They also provide strategies for coping with food insecurity (Dickin et al., 2021). Taking into account the influence of social and cultural norms on nutritional behaviors and the prevention of stunting encourages the adoption of integrated approaches (Wood et al., 2024).
Social Norms, Representations, and Practices Related to Growth
Child growth cannot be fully understood strictly in terms of biological parameters; it is also shaped by a social and cultural framework that profoundly influences individual trajectories. Implicit norms determine what is perceived as “appropriate” or “expected” development within a given group. They also guide breastfeeding practices, food choices, health risk assessments, and the use of healthcare services, which ultimately shape child growth trajectories (Dickin et al., 2021; Collaborative Network, 2019; Thuita et al., 2019). Society’s perceptions of children’s height, weight, and nutrition shape expectations at each stage of development. They influence the type and quantity of food provided, the timing of food diversification, perceived risks of undernutrition, and the distribution of parental responsibilities between men and women or across generations (Scott et al., 2026).
Understanding these norms, the mechanisms through which they exert influence, and the associated social sanctions is essential for designing interventions capable of changing behavior (Bicchieri & Penn Social Norms Training and Consulting Group, 2015). Gender norms are also important because they condition access to resources, available healthcare services, and nutritional information; they influence the distribution of domestic tasks and shape household decision-making. Analyzing these social and gender aspects often helps identify invisible barriers that hinder the adoption of recommended feeding practices.
Studies show that gender inequalities can limit access to food and the quality of nutritional practices (Mphangwe et al., 2024), while a greater mother’s autonomy is associated with improved nutritional outcomes (Eom et al., 2024). These findings underscore the importance of qualitative approaches for understanding social and cultural logics (Odii et al., 2024), as well as how families define and protect healthy child growth (Querre, 2007) in constrained material and environmental contexts.
Climate change increases children’s nutritional vulnerability, with a close link between the climate crisis and the global food crisis (UNICEF, 2023; Klapka et al., 2024). Extreme temperatures, floods, heatwaves, and variable rainfall intensify food insecurity (WHO, 2022) and malnutrition among children under five (Agabiirwe et al., 2022; Sparling et al., 2024; ST4N, 2025). In Senegal, these hazards disrupt agroecology, agriculture, food security, and water access, thereby increasing the risk of child malnutrition (Ndao & Breuer, 2013; Sy et al., 2022). Temperatures above 35 °C are associated with an elevated risk of stunting (Niles et al., 2021). The effects of rainfall are more nuanced: decreased rainfall can, depending on context, either worsen or improve nutritional status (Seposo et al., 2025). While reduced rainfall often compromises agricultural production and food security, it can, in certain environments, reduce exposure to waterborne and vector-borne diseases, such as diarrhea, cholera, or malaria, which affect children’s nutrient absorption and child growth.
Due to their immaturity and food dependence, children are particularly vulnerable to these health and nutritional effects (Thiede & Strube, 2020), as well as to the transmission of infectious diseases. To analyze stunting, it is essential to consider families’ perceptions of climate risks as well as the strategies they implement to prevent or adapt to them (Cooper et al., 2019; Macheka et al., 2022). They assess the nature of perceived risks, their priority, and the practices to adopt in response. These social representations shape behaviors related to agriculture, food, and health. For example, influencing crop selection, stock management, and responses to environmental shocks (Moreno et al., 2023). These dynamics play a structuring role in household food security and, by extension, in child growth and development.
Research Objectives
This study explores the interaction between social norms, socio-economic processes, and environmental factors to explain childhood stunting in Senegal, with a particular focus on the perceived impact of climate change. It also examines the vulnerability process that exposes children to chronic malnutrition, as well as the adaptation and resilience mechanisms mobilized by households and communities in response to these challenges. The objective is to gain a better understanding of the complexity of these dynamics and how they influence child development. Specifically, the study seeks to:
- Analyze explanatory models of child nutrition by integrating emic, socio-territorial, and environmental dimensions to identify interactions between cultural factors, social dynamics, and ecological constraints;
- Document social representations and local interpretive frameworks regarding the causes of stunting, highlighting the cultural and community logics that shape these perceptions;
- Examine parents’ perceptions of climate risks and analyze their influence on child care, feeding, and protection practices;
- Describe and analyze family resilience strategies in response to climate change, as well as the perceived effects on child growth.
Materials and Methods
This article presents a qualitative study on childhood stunting in Senegal, aiming to analyze the sociocultural, environmental, and community factors that influence feeding practices, caregiving, and the growth of young children.
To capture ethnocultural and geographic diversity, an ethnographic approach was adopted. The territory was divided into five socio-economic zones (Diouf, 1994). One region per zone was selected based on stunting prevalence and the presence of the PIPADHS program (Map 1).
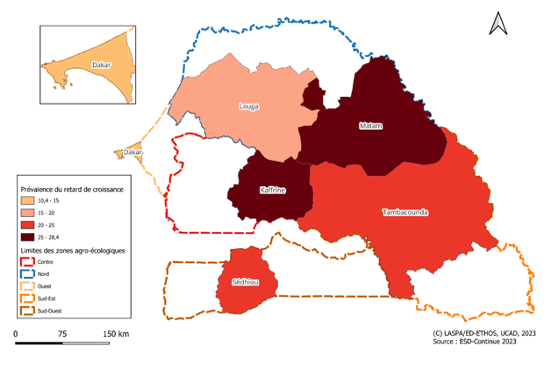
In each region, the department with the highest stunting rate was selected, followed by one urban and one rural municipality to ensure representation of different living environments. Two categories of participants were included. First, we targeted caregivers who had resided in the study area for at least 12 months and lived in households with a child under five. This term refers to mothers, grandmothers, fathers, and community health workers who are responsible for the nutritional and health management of children. Their role includes feeding practices, hygiene, childcare, disease prevention, and access to healthcare. These practices are embedded in an extended family framework, in which women play a central role. Second, key informants (health professionals, community actors, members of non-governmental organizations, and local leaders) were included. Minors (under 18 years of age) were not included in the study. The protocol was approved by the National Ethics Committee for Health Research in Senegal (SEN 23/107). All participants provided informed consent after being briefed on the study objectives and their rights.
We employed multiple qualitative methods to collect data. We conducted semi-structured interviews (n = 134 participants), which allowed us to better understand participants’ perspectives on child growth, feeding, and caregiving practices, and the sociocultural and environmental factors influencing them. Data saturation was reached after approximately 25 to 30 interviews per site. To identify childhood illnesses considered priorities by parents, appropriate foods, and key challenges for healthy eating, we conducted a free listing exercise with participants. Additionally, we held focus group discussions (n = 24) with parents, grouped by gender and experience with stunting. Finally, direct observations in households complemented the analysis by documenting daily behaviors related to nutrition, hygiene, caregiving, and family interactions.
The data analysis was conducted using ATLAS.ti software. After anonymization and secure storage, transcripts were first subjected to open coding to identify main categories emerging from the empirical material. This initial step was followed by axial coding, which allowed us to link the identified themes and structure the data around key dimensions: feeding practices, caregiving trajectories, and social and environmental determinants. Two researchers independently coded the data; any discrepancies were discussed and resolved by consensus. A cross-sectional comparative analysis was then conducted to identify variations based on ethnocultural contexts, type of environment (urban or rural), and category of actors involved.
Results
Understanding Childhood Stunting through Local Perceptions
- A social reading of child growth
In Senegal, child growth is understood in terms of the “healthy child,” which is reflected in height, weight, and developmental milestones such as the emergence of baby teeth, walking, language, or puberty. Satisfactory growth depends on caregivers’ response to basic needs, including nutrition, protection, and bodily care: carrying, massages with shea butter or touloucouna oil, and hydration. Carried out by mothers, grandmothers, or massage therapists, these practices shape the body according to social norms, transmit hygienic, therapeutic, and symbolic knowledge (Mbaye et al., 2021), and protect against invisible threats (Weber et al., 2010). Such caregiving practices and rituals demonstrate that child growth is a process shaped by social and cultural dynamics (Amoussou Lokossou et al., 2021).
- Domestic hygiene, environment, and caregiving dynamics
Across all study sites, women closely link children’s health and growth to the cleanliness of their domestic environment. They emphasize the importance of frequent bathing, regular clothing changes, cleaning the child before breastfeeding, and avoiding street food, all essential strategies for preventing childhood illnesses.
Parents also recognize various environmental risks, such as sandstorms, smoke from bush fires, street food preparation, pollution, and open-air burning of household waste. These practices can lead to respiratory and digestive problems in young children. Aware of these dangers, parents remain vigilant; however, economic and material constraints limit their capacity to respond. Increased father involvement, particularly in vaccination follow-ups, seeking healthcare, and providing financial support, is reported as a factor contributing to household stability and resilience. However, gendered role distribution remains predominant, with mothers bearing primary responsibility for children’s daily caregiving and feeding.
- Bodily practices and gendered socialization from early childhood
In Senegal, child growth assessment primarily relies on knowledge related to health, nutrition, and protection, transmitted mainly by women. According to them, ensuring a child’s health and vitality requires adherence to bodily and social norms that shape the body. For example, massages with shea butter or touloucouna oil help mold the child’s body according to societal criteria. These practices vary depending on the child’s sex:
I practice body-massage techniques to tone the children’s bodies. If the child is a girl, I use upward strokes during the massage to slim the waist and round the buttocks. For a boy, I apply pressure on the buttocks and smooth the lower abdomen. This aims to prevent excessive weight gain and strengthen masculinity. (62-year-old grandmother, Louga).
These practices highlight the meaningfulness of bodily care and its essential role in child growth and preparation for adult life. Women — mothers, grandmothers, aunts, sisters — play a central role in these childcare practices and the transmission of knowledge regarding nutrition, protection, and bodily care (Wallace et al., 2022). They also embody the early inscription of gender norms, with women primarily responsible for caregiving and men for financial support. However, fathers’ growing involvement in certain aspects of health monitoring suggests a partial reconfiguration of parental roles. Moreover, stunting is often interpreted as a result of parental negligence, typically attributed to mothers: some are perceived as lacking attentiveness or diligence in feeding and caring for their children, which might explain their children’s weakness or thinness. Thus, children’s health and balanced growth deeply reflect women’s dedication and expertise in their caregiving role (Wentworth & Blalock, 2025).
Neglecting factors such as economic precarity, domestic workload, or limited access to resources, these perceptions reinforce gender inequalities in child health care. This highlights the importance of understanding these obstacles in order to better support all families.
- Local causes and nosologies of childhood stunting
In Senegal, caregivers of children under five interviewed in this study use vernacular expressions such as Maggaay bu dàmm (interrupted growth), Xel mu fassu (constrained mind), Xorido mawnu (memory problems), Kondi (short stature), and Timpato (frail child) to describe stunting. These terms reflect four main interpretive axes: visible physical traits, apparent clinical signs (fatigue, abdominal swelling, lethargy), cognitive or behavioral changes, and causal explanations involving spiritual, genetic, or deviations from social norms.
Maggaay bu dàmm, (interrupted growth) a broken growth, xel mu fassu. If, at the same age as peers, others grow and he remains the same height, it is clear he is not growing normally. Often, his concentration is also affected (father of 2-year-old children, Boulal, Dahra, Louga)
Beyond height, parents evaluate a child’s growth by observing the general body appearance, behaviors, and motor or intellectual development. While corpulence is often valued, thinness does not necessarily indicate stunting: in central-western regions, it is often associated with illness, whereas in the north (Matam), it is regarded as a symbol of Pulaaku identity, representing endurance (Chevé et al., 2023). Similarly, in Tanzania, short stature is seen as natural or hereditary (Mchome et al., 2019), and in Ghana, children’s corpulence is not a cause for concern, but rather a sign of a prosperous family situation and parental care considered adequate (Ewusie et al., 2025). This social valorization of a “well-fed” body can make thinness less visible as a health problem and may delay the implementation of care or preventive measures (Pradeilles et al., 2022).
Furthermore, for parents, although stunting and malnutrition may present similar clinical manifestations, they are not considered to have the same etiology: malnutrition is mainly linked to insufficient or inappropriate feeding, whereas stunting is understood as a global condition associated with hereditary, mystical, or social causes. It represents a disturbance of the child’s body and intellectual capacities and raises questions about the types of interactions the child has with their environment, as well as the forms of interactions with the mother from gestation.
Indeed, gestation is considered a particularly fragile period, during which the fetus may be exposed to invisible influences that can cause anomalies or hinder its development:
Silouhoulein Yamouta is a childhood illness believed to result from a pregnant woman encountering a red monkey, causing growth disturbances and mental impairments. Among the Joola, it is described as a “bad wind” entering the pregnant woman’s body, particularly at dusk, causes Adjiomp Deum. Considered haunted by evil spirits, the mother would give birth to a child with stunted development. (52-year-old man, Sédhiou)
Associated signs include a frail appearance, wrinkled skin, sunken eyes, and a reserved or withdrawn demeanor. Remedies often involve ritual practices: special baths, wearing a cloth representing the monkey’s tail, and the mother mimicking the animal’s movements to ward off the spirit believed responsible for the disorder.
Additionally, the absence of certain childcare practices during early childhood, such as massage, anointing oiling, and carrying, is often considered a cause of growth disturbances. These practices are seen as highly protective, aimed at promoting growth, vitality, and safeguarding the child against vulnerabilities. The findings indicate that parents perceive stunting through visible signs in the child’s body, behavior, and social interactions within familial and cultural environments. However, these perceived manifestations, which draw on local knowledge, often remain partially invisible to biomedical nutritional tools, which contribute to limiting their recognition.
Child Nutrition: Between Cultural Norms, Maternal Practices, and Socio-Environmental Vulnerabilities
- Infant feeding practices
Rooted in local traditions, infant feeding practices depend on socio-economic constraints and resource availability. Traditional foods (such as porridges, couscous, local sauces, and milk) reflecting local knowledge, continue to be valued both for their cultural identity role and their contribution to growth, even though they often differ from biomedical recommendations.
Among the Fulani people, laciri é cossam (corn flour porridge with milk) is considered an essential food for children, as it contributes to their cognitive development and is readily available. In southern regions, staples include couscous (millet, maize, or sorghum), fondé (millet porridge), sombi gerte (rice and peanut porridge), and sombi mbox (maize porridge), all of which are widely available cereal-based foods. In the east (Goudomp, Diattacounda), common foods among the Diola include white rice, bissap (sorrel leaves), Bantabrosse (baobab leaves), and Kaldu (rice with fish sauce). In northern regions, milk, porridge, and couscous are preferred, often combined with monkey bread to prevent digestive problems. In Matam, however, feeding practices have shifted: milk, sorghum, millet, cowpeas, and lake fish have become scarce, prompting parents to buy supermarket products, which are often expired and potentially risky for children. This gradual introduction of market-bought foods is often perceived by health system actors as reducing nutritional quality.
For parents, maternal nutrition also directly affects child health. A well-fed mother produces nutrient-rich breastmilk, helping prevent malnutrition and other health issues, such as diarrhea. Breastfeeding and weaning practices, influenced by social norms, must follow appropriate practices (early initiation of breastfeeding, feeding techniques, frequency, introduction of complementary foods, food diversification, and food hygiene). Any challenges, whether due to cost, professional constraints, the consumption of low-nutrient beverages, or premature weaning, can negatively affect child nutrition.
Child Growth and the Environment: Community Resources, Risks, and Knowledge
- The environment as both a resource and a source of risks for child growth
The environment provides water, food, and medicinal plants, whose availability depends on preservation against pollution, overexploitation, deforestation, slash-and-burn practices, and the intensive use of chemical inputs. Parents associate poor water quality, unsanitary conditions, and pollutionwith childhood illnesses, risks heightened by environmental changes and climatic hazards (droughts, storms, fires), which increase nutritional vulnerability. Children often grow up in environments where close proximity to animalsandlimited access to water increase contamination risks.
For the parents interviewed, the immediate environment is perceived as a concrete living space, combining opportunities, practical challenges, and locally developed skills. They directly link its deterioration to specific health risks for children: air pollution causing respiratory infections, floods triggering diarrhea, or heatwaves inducing dehydration and compromising breastfeeding. These conditions illustrate children’s vulnerability to climate change, which can affect their physical and mental development from early childhood. These observations confirm socio-ecological models of malnutrition, which view growth as the result of interactions between individual, family, community, and environmental factors.
- Local Perceptions of Environmental Hazards and Their Impact on Children
In the study areas, climatic changes have local names that describe their immediate effects: sopéeku alam bi (disruption of the natural order), sopéeku jaw ji (change in ambient air), sopéeku jamono ji (alteration of weather conditions), soppeku gancax gi (changes in harvests), Géej gi daffa aaye (raging sea) and Jàw ji daa tang (overheated air). Parents are aware that floods and air pollution cause waterborne and respiratory infections. They also know that irregular seasons, droughts, and extreme temperatures, increasingly frequent, reduce food production and make food storage more difficult. Such phenomena often lead to early weaning and the introduction of solid foods instead of exclusive breastfeeding.
I breastfed my child for a year, but not exclusively. He needed to drink, especially in this heat. On my mother’s advice, I started giving him other foods at four months. I know he has timpato because he is smaller than his peers, and I hope he will recover. My grandmother refuses to take him to the hospital, saying it is not a disease requiring consultation. (Interview, caregiver, Kanel)
- Perceptions of Climate Consequences on Child Growth
Parents perceive climatic disturbancesas a major factor in food insecurity and nutritional difficultiesfor infants. Air pollution, dust storms, and sand-laden winds have been linked to increased respiratory and intestinal infections, affecting children’s physical growth and cognitive development.
Daily experiences show that climate changes (rainfall, rising temperatures, floods, heatwaves) disrupt food production and food system availability. Yields for major crops, such as maize and wheat, are already decreasing, leading to higher food prices and limited access. Increasing numbers of families report monthly food insecurity, experiencing hunger at least once a month. In southeastern regions (Tambacounda, Kédougou), available food is often insufficient, forcing parents to reduce meal size and frequency, compromising children’s intake of essential nutrientsfor optimal growth.
In Dakar and Matam, natural disasters, such as floods and river overflows, have caused the separation of children from their homes, parents, or caregivers. These events are also traumatic, as children lose their familiar environment. Situations like these affect their growth and mental development: after last year’s floods, our house was destroyed, and we had to be separated. Some of my six children were sent to relatives while I stayed with my breastfeeding baby. The separation lasted over eight months. On our return, the house was heavily damaged, and my two-year-old had lost weight. He ate very little, stayed quiet, and did not want to play. He often talks about his fears. I can see he is deeply disturbed. (Interview, mother of six, Nguidjilogne, Matam)
In temporary relocation sites, limited access to water, sanitation, and adequate living conditions increases exposure to disease and environmental stress. Stunting thus emerges as the product of complex interactions between food insecurity, morbidity, psychosocial vulnerability, and environmental changes linked to climatic hazards.
Local Practices and Resilience Strategies Against Climate Change
The data collected indicate that communities implement various strategies to mitigate climate change effects on child growth and development, in response to food disruptions, limited resources, and constrained living conditions:
- Mobility and spatial organization
Several participants reported that women and children move seasonally to access water, crops, or more shaded areas. The use of temporary shelters that provide thermal comfort is also being considered to protect children from heatwaves.
- Nutritional adaptations
Households frequently adjust their eating habits by changing the frequency and composition of their meals, enriching local porridges with nutritious ingredients, and prioritizing certain local cereals to cope with limited food availability.
- Female solidarity and micro-transfers
Breastmilk sharing among women has been observed and is guided by norms of respectability, supporting mothers facing difficulties and ensuring children’s nutritional needs are met. In Senegal, a caregiver who adheres to local breastfeeding practices (duration of breastfeeding, timing and frequency of feeds, how the child is held during feeding, and a two-minute rest period after feeding to allow the child to burp, expel swallowed air, and prevent colic and regurgitation) is perceived as a caring mother and is accepted by her community. These transfers help prevent dehydration and ensure optimal child growth (Amzat et al., 2024; Giannini et al., 2021).
- Reorganization of daily activities
Children’s daily activities, such as helping to prepare meals, cleaning, household maintenance, fieldwork, fetching firewood or water, and tending animals, are adjusted to avoid their exposure to heat. Among adults, agricultural and domestic tasks involving children are reduced or reorganized.
These dynamics, often invisible in biomedical and nutritional frameworks, reveal both local capacities and gender inequalities. The division of roles directly influences nutritional and health resilience, highlighting the importance of integrating a gender perspective into interventions aimed at mitigating the impacts of climate change.
Discussion
In Senegal, childhood stunting remains a major challenge and is perceived as a multidimensional phenomenon, combining biological, social, and symbolic dimensions. Parents often trace its origins to pregnancy, influenced by social or mystical factors (Alendi et al., 2025; Sosseh et al., 2023), which places a moral responsibility on mothers, a perspective largely overlooked by biomedical approaches (Wentworth & Blalock, 2025). Anthropological studies show that current nutrition and health discourses shape the image of the ideal mother as the primary caretaker responsible for child health, which reinforces maternal blame when growth fails (Benasso et al., 2019). While classical models focus on nutrient deficiencies and infections during the first 1,000 days, communities adopt a broader perspective, including maternal nutrition, social norms, rituals, and climatic constraints. Stunting is therefore viewed as a social and moral process, where a child’s trajectory may be “interrupted” by symbolic as well as biological disruptions (Rakotomanana et al., 2024). The coexistence of these explanatory frameworks reveals both dialogue and tension between local knowledge and scientific models, highlighting the importance of integrating social norms to enhance the acceptability and sustainability of interventions.
Extreme climatic events exacerbate vulnerabilities in health and nutrition (Niles et al., 2021). While traditional models consider climate as a distant factor affecting access to food and healthcare (Thiede & Strube, 2020), Senegalese families incorporate it directly into feeding practices, care strategies, and household decisions (Agostini et al., 2023; Tamasiga et al., 2023). The findings of this study shows that child malnutrition cannot be reduced to biological deficits or isolated anthropometric measures. Children’s growth depends on complex and dynamic interactions between environmental, nutritional, social, and economic factors, closely tied to local climatic conditions (Santos-Degner et al., 2025). This socio-ecological perspective suggests that stunting arises from an ecosystem in which children’s individual pathways are shaped by local environments, social structures, and food systems. Climate change intensifies these challenges, worsening food insecurity. Understanding its effects on nutrition requires analyzing socioeconomic status, access to resources, and gender dynamics (Hanieh et al., 2020; Lucey & Grimm, 2021). Ultimately, child nutritional vulnerability stems from both structural and contextual factors, emphasizing the need for a holistic approach rather than purely biomedical interventions.
Despite these obstacles, households demonstrate ingenuity by adopting strategies that combine local food knowledge and community solidarity. By adjusting agricultural practices, diversifying crops, and strengthening social and family networks, some families manage to ensure stable growth for their children. This constitutes a domestic ecology of health, where daily routines and food choices interact with social norms to promote child growth within a specific context (Bricas et al., 2021; Frumence et al., 2024; Nedzingahe et al., 2023) while remaining constrained or influenced by socio-economic inequalities and contextual limitations. Households thus become spaces of resilience, where local knowledge and cultural practices maintain nutritional security despite environmental, economic, and health uncertainties (Scheidecker et al., 2025).
These mechanisms show that resilience is socially shaped, strongly linked to gender, and deeply rooted in local norms and skills (Laar et al., 2022). By valuing local knowledge, supporting family adaptation strategies, and carefully considering climatic and social constraints, positive change can be fostered. Nutrition initiatives should go beyond traditional biomedical frameworks to adopt a more integrated approach. This involves strengthening local food systems and integrating social and climatic dimensions, while ensuring gender equity for a more balanced future. Furthermore, these findings invite a rethinking of nutrition in Africa, moving beyond imported paradigms to value and integrate local knowledge, traditional feeding practices, and community perspectives (Louvin & Walser, 2021; Swiderska et al., 2022). As Nelson et al. (2021) note, the field of nutrition has long been influenced by colonial legacies (with Western dietary norms imposed as reference standards, nutrition policies promoting the consumption of imported or processed foods, and the reorientation of local agriculture toward export crops), international power dynamics, and technocratic approaches that prioritize technical solutions over social, political, and structural aspects of malnutrition. However, it should not be overlooked that, under the influence of socio-economic changes, dietary practices remain rooted in local knowledge while adapting to the challenges of globalization. These dynamics are often rendered invisible by conventional social and behavior change communication methods often rely on standardized models that do not account for ecological and social particularities, limiting their effectiveness (Faye & Sow, 2025). In contrast, a decolonial approach seeks to equitably recognize local knowledge, reintegrate the social, historical, and political dimensions of food, and promote community participation as well as the valorization of indigenous food systems (Jernigan et al., 2023). Integrating peasant knowledge into ecological practices is a strategy for promoting more context-appropriate food and nutrition systems (Moseley, 2024; Mougeot, 2006). Overall, these findings underscore the importance of developing participatory, contextualized nutrition interventions that consider domestic ecology, local knowledge, and social, cultural, environmental, and gender dimensions to strengthen community resilience and children’s food security.
Conclusion
In Senegal, childhood stunting cannot be reduced to a simple nutritional problem; it primarily results from the interaction of diverse socio-economic, cultural, and environmental factors. In particular, social norms related to pregnancy and childcare practices shape the expected maternal behaviors, as well as the risks associated with mystical perceptions about child health. These norms also guide how the child’s growth and health status are perceived. They are not obstacles to adopting biomedical food recommendations; rather, they constitute coherent systems that adapt and self-regulate. Understanding stunting requires grasping the social, cultural, and environmental dynamics that shape child nutrition. Socio-ecological approaches show that malnutrition arises from a complex web of interactions between food systems, social inequalities, gender relations, and climate change, with the latter acting as an amplifying factor of household vulnerability.
To make nutrition interventions effective, it is essential to integrate scientific data, local knowledge, social norms, and responses to environmental pressures. By valuing local knowledge and respecting traditional feeding practices, while also incorporating gender considerations and ecological sustainability within families, such initiatives can strengthen household resilience and sustainably improve children’s nutritional security in Africa.
Acknowlegments
The authors express their deep gratitude to all participants (caregivers, key informants, local authorities, and community actors) for their availability and valuable insights, which greatly informed this study. They also thank the field teams (Paul Mamba Diédhiou, Ousseynou Diouf, Aliyou Talla, Henriette M. H. Ndong, Khadidjatou Sankhe, Abdoulaye Ndoye, Diabou Diao, Cheikhna Cheikh Saadbou, Seydou Bachir Sarr) for their commitment and rigor in data collection.
This research benefited from financial support from the CNDN, which was crucial for the completion of this work. The authors remain solely responsible for the content and analyses presented in this article.