
Context
On March 2020, the 12th, the first case of Covid-19 was recorded in Conakry[1] when a European Union official arrived in Guinea after spending time in Belgium and France for her holidays. At the time Covid-19 presence was acknowledged in Guinea, the country was just emerging from the trauma of the Ebola virus disease. It also coincided with a period of socio-political crisis following the organisation of a contested constitutional referendum authorising the President of the Republic, Alpha Condé, to lead an electoral campaign and to be elected for a third consecutive term. The elections led to a sense of politicisation of Covid-19 (Kamano, 2020). Many people perceived the implementation of barrier measures such as the curfew and the ban on authorised gatherings in markets as a conspiracy from the government, arguing that these health measures were in fact aimed at muzzling political demonstrations.
In the early hours of the pandemic, all those who were tested and identified as positive for Covid-19 (whether symptomatic, paucisymptomatic or asymptomatic) were quarantined in dedicated sites and placed on treatment. This situation was inspired by the Ebola response, during which treatment centres were automatically established from the start of the epidemic, both to cure positive patients and to contain the spread of the virus in the country (Gomez-Temesio & Le Marcis, 2017). These treatment centres were frequently described as places of death (‘mouroir’) (Mbaye et al., 2017). Concerning Covid-19, the quarantine of positive patients was similarly perceived as imprisonment. In particular, asymptomatic individuals rejected their infection and questioned the need for treatment (Attas et al., 2021). As a result, the relationship between the population and healthcare staff became increasingly challenged and conflictual, involving arguments, escapes, destruction of healthcare facilities and refusal to observe treatment. This relationship between patients and caregivers echoes the particular relationship between the Guinean population and the authorities (Gomez-Temesio & Le Marcis, 2017), defined by a lack of trust (Somparé, 2020). In this context, the management of the pandemic is perceived as a tool of oppression (Attas et al., 2022, p. 28). Implementing quarantine for Covid-19 positive patients, the government was suspected of intending to poison people, especially in opposition strongholds. This perception is not specific to Guinea; it has been observed in other African countries. In Uganda, for example, Melissa Leach et al. (2022, p. 10) mentioned that the quarantine or forced hospitalisation of asymptomatic patients has led to discussions about the government’s alleged intention to poison political opponents. In Guinea, this level of mistrust resulted in the refusal of Covid-19 testing, non- compliance with sanitary measures, and street demonstrations – all factors which strongly contributed to spread the virus among the population. In June 2022, the 19th, the country had 37,123 confirmed cases, 443 hospital deaths, and 338 positive community deaths (ANSS, 2022)[2]. Conakry accounted for 80% of confirmed cases and had a 60% general population infection rate (Soumah et al., 2022). On the basis of this observation, I asked myself what factors, particularly social factors, expose people to the risk of Covid-19 contamination. Why are preventive measures perceived in a mixed way by different actors? How is compliance with barrier measures a tragic choice between living biologically (healthy) and dying socially, or living socially and risking death? These questions are addressed using data collected between June 2020 and September 2021 as part of the research programmes:
‘Ebola’s shadow on the SARS-CoV-2 epidemic[3]’ and ‘Dynamics of the SARS-CoV-2 epidemic in Conakry, Guinea (COVEPIGUI)[4]’ . In this seroprevalence study, I conducted an ethnography study based on open interviews and repeated observations in the households of people identified as Covid-19 positive. I reconstructed the conditions of infection through a retrospective study supported by a descriptive approach. The identities of the respondents were anonymised, information allowing them to be identified was modified and the necessary sociological elements were retained. The names and addresses mentioned in the text are fictitious, but plausible.
I first present the key elements of the difficult management of Covid-19 crisis, as well as the variety of circumstances and conditions under which people are infected (as they appear from a material point of view, but also as individuals perceive them). However I do not claim to categorically explain the origin of the contaminations. This exercise demonstrates how the experience of contamination is both an objective and subjective reality. Secondly, I propose to analyse the notion of ‘social network’, a provider of opportunities but also a risk factor for contamination in a context of health crisis in Guinea, where the welfare State and an adequate health system are lacking (Diakité, 2016; Somparé, 2017; Diallo, 2021). Finally, in the last section, I discuss Covid-19 in Guinea to address the tension between the biological and social being. The respect of barrier measures to preserve biological life entails a risk for the maintenance of social life, even though the latter guarantees individuals’ resources and means of survival or of responding to possible health difficulties they may encounter in the absence of adequate State response. In doing so, I pay particular attention to people’s perceptions of barrier measures.
Covid-19: a highly mobile disease that defies popular belief
The emergence of Covid-19 has taken the world by surprise, as if this kind of sanitary crisis was outdated and only concerned the great health crises of the Middle Ages (Misturelli, 2020). The first suspected case was recorded on November 17, 2019, in Wuhan, Hubei Province, China (Dumont, 2020) and officially declared by the authorities on December 23 (Offner et al., 2020). Containment was not enforced until January 23, 2020. The virus therefore had ample time to spread within the country and around the world (Dumont, 2020), following the movements of international travellers (Lemey et al., 2020). Improved transportation, which favours the hypermobility of people, has served as a medium for the spread of Covid-19. It would have remained strictly ‘Chinese’ if China, particularly Wuhan (the epicentre of the disease), was not highly connected to other cities in the country and in the world through its various transport networks (Dumont, 2020). By the end of the first quarter of 2020, Covid-19 had affected many countries, posing a threat to global health and security. On March 11, 2020, deeply concerned by the rapid spread and severity of the disease, the World Health Organization (WHO) declared a global pandemic (WHO, 2021). At the beginning of the pandemic, some people considered the disease a distant threat (Goulard ,2019), or believed that it would not affect their locality. This belief was soon challenged. Deeply affected by the Ebola virus epidemic that hit three Mano River Union countries (Guinea, Liberia, and Sierra Leone) between March 2014 and March 2016 (Gasquet- Blanchard, 2017; Gomez-Temesio & Le Marcis, 2017), the Guinean society incredulously watched the evolution of Covid-19 at international level with concern. While anticipating to escape the virus, it experienced the pandemic with the rest of the world (Sylla, 2020). In the early days of the disease, international travellers and senior government officials were the most affected. They were perceived as being most at risk and responsible for the transmission of the virus. A part of the population did not feel concerned by the disease and considered that their socio-economic situation would allow them to escape it, as it reduced their exposure to the risk of viral contamination. An elderly Malinké woman living in the suburbs of Conakry said: “We know the people who contract this diankaro djou (bad disease). We won’t get it, because there is no condition that exposes us to it”.
A retired civil servant, met at the end of May 2021, wondered:
“From what we see and hear via the media, Covid-19 is serious. But it is impossible to contract it if you don’t travel abroad (Asia and the West) and if you are not an executive who attends meetings. I spend my whole day between the mosque and home. How can I get it in this situation?”
During the first four months of the outbreak, the communes of Dixinn and Ratoma, home to expatriates, senior civil servants, large traders and/or businessmen, had the highest rates of infection, as shown on Map 1.
However, despite the measures taken and the political will to contain the spread of the virus, all of Conakry’s districts – with contrasting socio-economic profiles – were affected after several months. Beyond the capital city, Covid-19 spread to several towns in the interior of the country (see map 2 below). During the month of September 2020, observers mention a “community transmission” (MVAT/ DATU & UN-Habitat, 2020) that affects all strata of the population. The spread of the Covid-19 virus in Guinea therefore has been vertical and downward, from the elite to the most downtrodden social strata. Preventive measures appeared are constraints that are difficult to respect as they hinder social practices that are widely shared in society.
Preventive measures against Covid-19: a threat to social life, yet a guarantee of biological life
On the 25th of March, the President of the Republic Alpha Condé declared Covid-19 a public health emergency. On the 18th of April, restrictive measures were issued (Cissé, 2020) by the Ministry of Health through the National Health Security Agency (ANSS) in compliance with the recommendations of the World Health Organisation (WHO). These measures comprised the introduction of a curfew; the promotion of regular hand-washing; the closing of places of worship and educational establishments; the prohibition, in absence of a negative test for Covid-19, of gatherings, commercial flights and travel between Conakry and the country’s prefectures; the reduction in the number of passengers on public transport; travel and visits to relatives (MVAT/DATU & UN-Habitat, 2020). These measures are part of a classic approach of health crises management (Diouf et al., 2021) and follow internationally imposed practices, which are more adapted to Northern countries (Casciarri, 2020) than countries of the Global South. In Sudan, for example, they have proved destructive in relation with local practices characterised by significant sociability and conviviality (Casciarri, 2020). In Guinea, they appear to be unsuited to people’s lives. Indeed, they force individuals to choose between zoe (the simple fact of living, or the physical life of the living being) and bios (the life of the human being as a political being, living in his or her own way both individually and collectively) (Dubreuil, 2005; Fassin, 2006). Or, in other words, to choose between the biological life and the social life. The distinction between these two definitions of life is less clear-cut in reality. For Guineans, maintaining a social life also means guaranteeing a biological life. Maintaining a social life implies constant socialising and interaction. Being part of a social network implies keeping company and interacting, and this registration allows one to benefit from moral and financial support when difficulties arise (loss of employment, problems with the law, domestic issues at home, health problems or even death, etc.). In the context of the lack of social safety nets in Guinea, refusing to participate in this network or avoiding interacting with and hosting relatives is to jeopardise potential support channels for an individual. Distancing oneself from loved ones in the name of managing an illness means losing their support in case of problems. A shopkeeper in his sixties said during the second half of 2020: “Personally, I cannot cut off my family and friends to avoid Corona. If I do so and then have difficulties, no one will come to my rescue”.
While Covid-19 remains a threat (WHO, 2021) elsewhere, the discourse on epidemic management in Guinea takes a completely different form: in local discourses, preventive measures are a form of economic and social ‘screwdriver’ and they are increasingly difficult to comply with for the population. They largely hinder local practices (Attas et al., 2022, p. 27), these latter constituting ‘social shock absorbers’ in the absence of which a large part of the population will find itself in difficulty. This belief motivates acts of resistance against restrictive measures aiming to control the spread of Covid-19. As a result, actors prioritise social life to the detriment of applying recommended health measures. Based on four case studies, I first report on the link between social role within one’s local network and exposure to the risk of Covid-19 contamination. Two contrasting examples are discussed: a person with a high social status and a person with a low socio-economic status. I then discuss the difficulty of preventing Covid-19 due to objective living conditions, and then in relation to living arrangements. In these different cases, preventive measures are blind to local contexts and disconnected from local realities.
Social networks are a source of opportunities and risks during a pandemic
The notion of a social network today evokes the digital world (Facebook, LinkedIn, Twitter, etc.); however, this is only one of its specific forms (Kiyindou, 2011). A social network refers to a group of individuals who maintain diverse and varied links (Mercklé, 2016). As welfare State does not exist in practice in Guinea, people focus on networks of belonging to solve their problems. They also focus on these same networks to obtain financial, material and health support. The social network thus constitutes a social net, one of the main forms of social protection that facilitate access to resources (Marie et al., 1997; Bidart et al., 2011). It implies logics of reciprocity, constraint or obligation, making individuals accountable to each other. In Guinean society, members of a network are obliged to participate in each other’s social events (hospitalisation, wedding, baptism, funerals, etc.). Anyone refusing to do so while they have financial or material means will be ostracised by the members of their network and they risk receiving no support when they will be facing difficulties of any kind. In this context, individuals come to put themselves at risk in a health crisis situation (Faye et al., 2015). Numerous Ebola contaminations occurred during the fulfilment of obligations within the network (WHO, 2014; Thys & Boelaert, 2017; Desclaux & Barranca 2020), as well as Covid-19 contaminations (Galmiche et al., 2020; Dumont, 2020). The case of Marie and her niece, both tested Covid-19-positive, demonstrates how the fulfilment of obligations within the network allows for exposure to the risk of contamination.
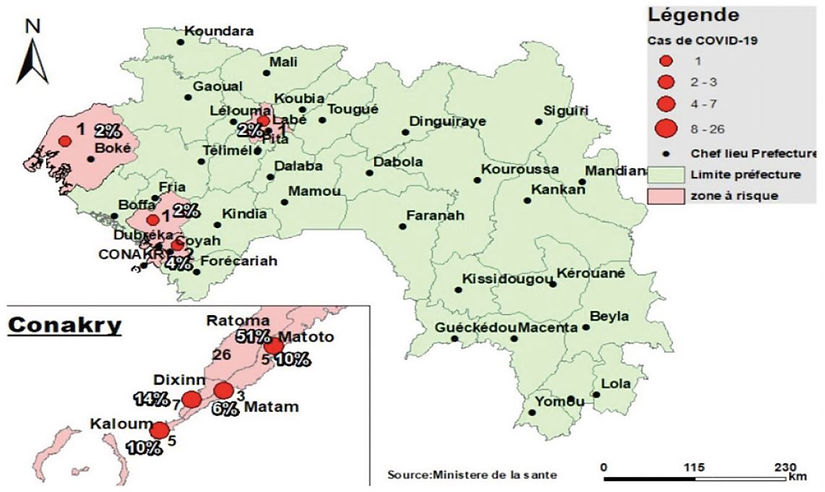
Map 1: Spatial distribution of confirmed Covid-19 cases in Conakry and Guinea from March 12 to June 5, 2020 (source: Ministry of Health 2020)
Marie has been a widow for six years, she is a small trader selling local rice at retail. She lives in a communal courtyard in Tâkhoui[5] , a sub-district in the commune of Kaloum. In July 2020, she and some members of her extended family travelled to Nzérékoré (a town 864 km from Conakry) by intercity public transport to attend the funeral of her older brother who died after a brief illness. At the time, to contain the spread of the virus, there was a ban on travel between Conakry and other national cities. Marie’s brother was a priest and well known in the Nzérékoré’s region. He was the “baobab”[6] of the family and an important support for her, she says. His funeral was an important gathering of his relatives from all over the world. It was also a time of intense exchange between visitors. Few of them applied the sanitary measures, she explains. Women are more involved in ceremonies or social gatherings (Dessertine, 2021). Marie spent two weeks in Nzérékoré. During her stay, she and her sisters, assisted by relatives, were in charge of welcoming visitors and cooking. On her return to Conakry, she developed a cold and muscle pains. She believes that she came into contact with the virus during her stay: “I contracted this disease during my trip because I was widely exposed”.
In order to understand the supposed logics of Marie’s infection, it is necessary to understand how economic status and gender intertwine. After a long collective journey by car, in order to ensure the reception and preparation of meals because of her status as a woman, Marie found herself once again immersed within a crowded group. Marie’s refusal to attend her brother’s funeral would have been frowned upon by her relatives, who would therefore not help her if she found herself in health, social or economic difficulties. Thus, fulfilling obligations within the network helps to avoid the danger of exclusion and is vital in a situation without social assistance provided outside one’s personal network. In addition, in order to secure their network even more, women actively insert themselves into the larger social space by maintaining, beyond the parental sphere, a network of relationships such as contractual associations (Marie et al., 1998). This is the case of the sèrè, a type of women’s organisation that is widespread in Guinea, characterised by mutual aid, tontines and regular meetings between members. These meetings contribute to the exposure and spread of the epidemic. Marie’s niece also tested positive for Covid-19. She is a sixteen-year-old girl: her parents live in Nzérékoré and she was placed under Marie’s care when she was younger. “Confiage” or the circulation of children from one family to another is an ancient practice, very widespread in African societies (Jacquemin, 2000). Some actors resort to “confiage” to strengthen family solidarity. Others do it for personal interests by transforming the girl into a ‘little maid’, so that she participates in housework (Vidal, 2013) and in certain economic activities (Jacquemin, 2000). Together, Marie and her niece prepare meals and they share the same plate of food when they are both present at home. The niece maintains the house, washes clothes and often joins her aunt at the market to assist her in her business activities. The niece believes she contracted the virus in their interactions, stating:
“I think [I] came into contact with the virus when I was with my aunt. In addition to the interactions at home, I often join her at the market to help her sell rice. I serve and collect money from customers”.
In Guinea, young girls generally perform tasks such as assisting with meal preparation, laundry, cleaning the house and washing up. These tasks involve staying at home and do not necessarily involve contact with other people. However, beyond housework, Mary’s niece helps her with her business. This puts her in a situation of constant interaction with other people, which also contributes to her exposure to the virus. She has come into contact with the virus because she is in a service situation and occupies a lower position in her network.However, other people with a high position in their network also come into contact with the virus because of their role.
Assume Kountigi (village elder)’s role at the risk of contracting the Covid-19 and spread it
The role of the Kountigi is held by the founding family of the village. The Kountigi is the ‘moral authority’ and the ‘guarantor of peace’ in the village. He mediates between the protagonists and coordinates social activities. He relies on a network of chiefs from the main families in the village to carry out his functions (Bernus, 2005). Thus, the Kountigi is in frequent interaction with several people: the members of the council of elders (direct collaborators) and the inhabitants of the village. This situation is conducive to getting contaminated by Covid-19. It was the case for Elhadj, who tested positive with four members of his family at the end of May 2021.
Elhadj lives in the commune of Ratoma, in N’nôma[7] , an upscale residential area. A retired civil servant, he lives on his pension, the profits from his cashew tree plantation and the help provided by his children. As the oldest within his family, Elhadj is the Kountigi and presides over the village council of elders and the association of members of his village residents in Conakry. “At my age, I only deal with social issues and maintaining peace in the village. It is at my house that we organise all our meetings”, he says. As a result, his many responsibilities require him to travel and interact with other people all the time, which increases his exposure to the epidemic.
During the first months of the pandemic, Elhadj organised religious weddings and baptisms – moments of conviviality and reunion including many people. He also attended the funeral of his brother-in-law, which took place in the village, and organised the funeral of his first son who died in Conakry. On the occasion of these funerals, relatives living in the village, neighbours and friends, came in large numbers to offer their condolences and express their sympathy to the family. Some of them stayed at his home for several days.
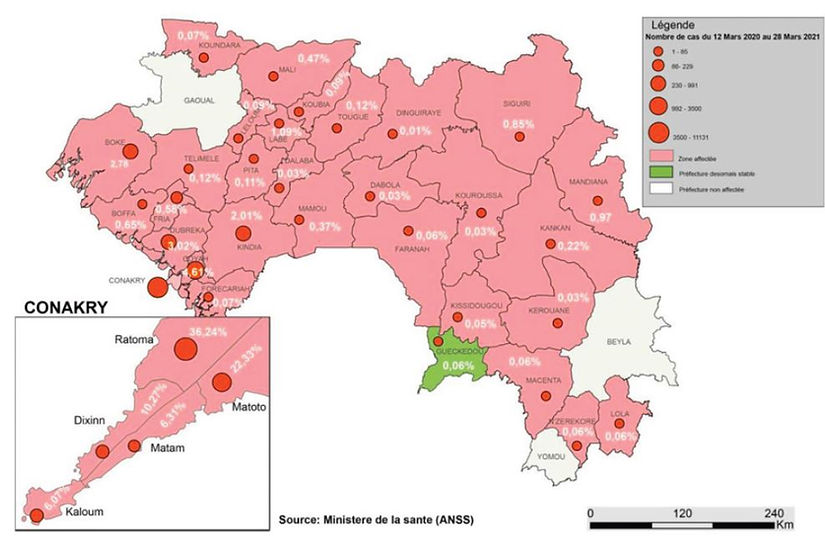
Map 2: Spatial distribution of confirmed Covid-19 cases in Guinea from 12 March, 2020 to 28 March 2021 (Source: ANSS 2021)
Funerals are an occasion for people to come together and are an expression or a display of the social weight of individuals. They give a concrete demonstration of the extent of the family’s social network. In so doing, they reinforce sympathy, affection and the bonds of solidarity that exist around the deceased (Le Marcis, 2015). They are also opportunities to assess the degree of esteem that individuals have for the bereaved family (Abdou, 2013). During funerals, some people who share common interests are seen chatting in private. Others, especially the elderly, sit together in one place to discuss and make decisions collectively. This situation is very conducive to Covid-19 contamination. After these events and ceremonies, Elhadj developed a dry cough, severe headaches and lost his tasting abilities. He suffered from breathing difficulties and could not walk more than fifteen to twenty metres without stopping several times. His wife, who often spent the night by his side;̵ his brother, who was at his bedside; but also his daughter-in-law, who looked after him with regard to food; also developed signs of Covid-19. But none of them agreed to be tested in order to find out the true nature of their illness. They have all resorted, says Elhadj, to self-medication by combining modern (tablets) and traditional (herbal teas) treatments. Self-medication is widely shared in Guinean society. On a daily basis, patients use modern and traditional medicine simultaneously or successively to treat their illnesses (Le Marcis et al., 2021, p. 42). Self-medication is common in Guinea, but it has become more widespread since Covid-19 health crisis. For Elhadj, Covid-19 is an unavoidable disease, which can be contracted anywhere and at any time, and which can only be prevented by divine power. He assumes that he contracted the disease and spread it within his family as a result of his participation in the above-mentioned events.
He explains:
“It is now clear to me that I was suffering from Covid-19 which I surely picked up [contracted] from the ceremonies, funerals and meetings I attended at the time. I came and contaminated my family. Covid-19 is dangerous, but it is impossible to prevent it”.
Elhadj has decent living conditions in terms of housing and material and financial means that should allow him to properly apply or follow the recommended health measures. However, despite the recognition of the dangers of Covid-19 on the national territory, he continued to perform his duties, maintain his usual travels and interactions. His perception of Covid-19 as an ‘unavoidable disease’ and his status and role within his social space are important factors in his failure to comply with preventive measures. As the person in charge, taking the risk of prioritising health measures to the detriment of the functions he performs in the network would have a negative impact on the proper functioning of the network, as it would be viewed and interpreted incorrectly by the members. Therefore, compliance with these measures is inappropriate for Elhadj’s profile. In addition, beyond perceptions and social status, the data collected showed that some people are exposed to contamination due to their living conditions.
The districts on the outskirts and the difficulty in preventing Covid-19
For the past twenty years, several neighbourhoods in Conakry have been subject to strong socio- demographic pressures (Kébé-Gangneux, 2016) which have led to an uncontrolled expansion of the city. Individuals built in certain areas without a real regulatory plan (Somparé, 2020) and without an adequate management of the space (Kouadio Oura, 2012). This situation is very favourable to viral circulation, as it is in Tâfori, a densely populated district on the outskirts of Conakry. The alleys are quite lively: the doors and windows of the houses open onto the street and, in front of them, people sit, chat, eat, and sell fritters without any sanitary measures being applied. Tâfori, which means ‘old village’ or ‘old town’ is poorly planned in terms of urbanism, and access is very difficult by vehicle. It lacks sewers, so when it rains heavily, all the streets and most of the houses are flooded. Piled-up rubbish is often seen at crossroads, slowly burning or waiting for a hypothetical collection.
Housing is dominated by old houses without fences, built in banco, a mixture of coarse soil and water, with two to four rooms, a small terrace, blackened walls with faded paint, rusty roofs usually held together by pieces of wood, stones and used tyres. In each of the courtyards in the neighbourhood, the toilets are shared. The rooms are communally shared, housing three to four people who are generally members of an extended family, which, in addition to husbands, wives and children, includes grandchildren, nephews, nieces, brothers, sisters, cousins, uncles, aunts, etc. Sharing rooms is very common in large Guinean cities (Barry, 2006), and is explained by a certain level of humanism and solidarity (Janin, 2003), but also by the absence of affordable social housing and strong regulatory mechanisms to control rent. Tâfori has no drinking water system and no health facilities. Its inhabitants travel to consult a health worker in a neighbouring district and obtain water from other districts or from people who have a well in their yard. The latter are invaded by a procession of water carriers at any time of the day. The search for water is therefore the occasion for large gatherings of individuals from different families who ‘mix’ and ‘rub’8 with each other. In this context, there is an extreme level of promiscuity that exposes citizens to risk. Soumah, a retired teacher and husband of three women, is no exception to this situation. About twenty people make up his extended family. Among them, fifteen individuals have tested positive for Covid-19. He has a water pump at home. This is connected to the well of a (rich) neighbour who always closes the gate to his yard. Thus, the other neighbours (women and children), equipped with jerry cans and buckets, come to draw water from his house all day long. Some, waiting for their turn, sit on the terrace. Others remain standing and talk to each other. None of them wears a protective mask. The lack of basic social services is of much greater concern to the inhabitants of Tâfori than the prevention of possible contamination to Covid-19. Soumah wonders:
“What can we do to protect ourselves against this disease (Covid-19) when we live in a precarious neighbourhood where there is a total lack of infrastructure and social support, and where promiscuity and social interaction are important?”
Despite its high population density, Tâfori has no public spaces or equipped playgrounds. Such realities concern the vast majority of Conakry’s neighbourhoods: they are attributable to anarchic urbanisation and uncontrolled land use, preventing any urban renewal initiatives, especially in the slums (Diop, 2015). In Tâfori, the inhabitants spend their entire day crammed in the living room or on the terrace, without the slightest respect for preventive measures, including physical distancing. Most of the rooms are poorly ventilated, a situation that favours viral contamination. In addition to the lack of infrastructure, it should be noted that the vast majority of the inhabitants are financially deprived and live from day to day, which, moreover, has an impact on obtaining or using hygiene kits. Their daily life is marked by very dense interactions; in fact, the restrictive measures, especially the limitation of movements and visits to neighbours or relatives are unbearable for them. Without such interactions, some will find themselves in distressing situations. In addition to living in the periphery, staying at home also contributes to exposure to contamination.
In addition to living in the periphery, staying at home also contributes to exposure to contamination.
Sharing a home: a factor of exposure to the risk of Covid-19 contamination
Bangoura is a neighbourhood chief. He is commonly called Mènguè (chief ). He and ten other members of his family tested positive for Covid-19 in June 2021. They live in a small old house, which consists of four rooms with three to four people in each. They are occupied by Bangoura’s grandchildren, children and three wives (he does not have a fixed room, he alternates between the rooms of his wives every three days). The house also has a living room with plastic chairs and a flat-screen TV connected to the Canal+ TV package, in front of which the family gather in the evening to watch the news or a film. It also has a terrace that serves as a place to receive visitors, a place to meet and talk, a place to sell sandwiches, a kitchen and a dining room. There is a notable absence of hygiene kits, as well as intense promiscuity and interaction between family members, but also between them and the inhabitants of the neighbourhood. When the latter pass in front of the home, some stop to exchange a few words with the family. Others, who are more intimate, try to tease Mènguè and come forward to shake his hand.
Mènguè calls himself a jatigi (host) and yama higi (hope for all the inhabitants of the neighbourhood), and considers his home to be a ‘common house’, a meeting place that is not just for the family (Houssay- Holzschuch, 1998). The inhabitants of the neighbourhood come here to spend several hours watching television, sharing meals or talking with Bangoura’s family. His older children, who do not live in the house but consider it a ‘basic unit of belonging’ (Dessertine, 2021, p. 21), come to spend long periods of time there for various reasons: to check on their parents and younger brothers, to share meals with the family from the same plate. This time is an opportunity for closeness and exchange between family members; it is also a time for reminding them of the tasks to be carried out and for discussing issues of concern to the family (Brunet et al., 2013). Finally, it is a space for communicating behavioural patterns that express the values of the family network (Barou & Verhoeven, 1997), such as mutual understanding and respect between children. Moreover, suffering from prostate problems, Mènguè does not accept to be away from home for long. He organises meetings of the neighbourhood council there and receives residents for administrative matters and for resolving conflict situations. In Guinea, the neighbourhood chiefs (Mènguè) function as a first level of justice and peace; armed with regulations, they arbitrate disputes and mediate between the protagonists (Wisler et al., 2018). They also participate in the management of administrative and health affairs (Kébé-Gangneux, 2016) in their locality.
One morning, while I went to his home, Mènguè was absent. His daughter, sitting on the terrace with a friend (a neighbour), informs me that he has gone, as usual, to the bar-café next door and invites me to sit down. An old woman and two young men are sitting waiting for Mènguè to return from an administrative consultation; five other young boys (neighbours and sons of Mènguè) are sitting and chatting amongst themselves, waiting for the girls to come out of the living room to watch a football match. On the low wall of the terrace sits Mènguè’s grandson, with three other little boys. He is playing with his grandmother’s (Mènguè’s first wife) telephone. She is sitting on a chair on the other side of the terrace, In front of her, a table is laid out with goods for sale: a bag of rice containing bread and two pots, one filled with beans and the other with stew, which local people come to buy for breakfast. Five customers queued up to be served. Like her, none of them wears a protective mask, uses hydro-alcohol solution, or respects physical distance. Dressed in shorts and a T-shirt, Mènguè and her secretary come to meet us on the terrace. Mènguè asks her granddaughter to bring two chairs for them. They sit next to each other. His grandson9 – his homonym always close to him – comes and sits on his lap. Then they start to talk with the old woman and the two young people who were waiting for mènguè. Again, no one wears a protective mask or respects the physical distance. While they are talking, a young woman comes without a protective mask to ask for a residence certificate10 ; Mènguè signs it before handing it to the young woman. It starts to rain later, and Mèngue invited all his guests to join the living room, despite its limited size. Some stand. Others sit on chairs in the room. At this point, there are about fifteen of us gathered together, none of us wearing masks: maintaining any physical distance is simply impossible.
“I am informed about the realities of Covid-19 through the media and the people I meet. But, I am yama higi. Everyone comes to me to solve their problems; it is very difficult for me to stop this. As a local leader, the further away you are from the people, the more you are hated ”.
The prevalence of Covid-19 has not changed anything for Mènguè. Yet he is informed about the pandemic. The management of Covid-19 is a minor concern for him compared to his local status. Here clearly appears the difficulty of making local officials strong and necessary actors in the prevention of epidemics without questioning the very nature of the epidemic. Preventing contamination for Mènguè induces that he would no longer assume his social role. While local officials have, in some places, demonstrated great effectiveness during previous epidemics, notably with Ebola (Mbaye et al., 2017), the reproduction of the same mechanisms without taking into account the nature of the Covid-19 virus appears questionable. Furthermore, the spread of the virus within Mènguè’s family can be explained by the impossible respect of barrier measures and the material conditions of habitat, subsistence, his wife’s (commercial) activities, visits and close interactions within the household, but also by responsibilities and social status.
Conclusion
Since the beginning of the Covid-19 pandemic in Guinea, the authorities have taken measures to prevent the spread of the virus. However, the socio-political context in which the disease has spread and the tough living conditions of the population of Conakry have undermined the application of these latter. Barriers measures clashes with values and practices that are well established in Guinean society, including ordinary interactions and the fulfilment of social obligations. Compliance with restrictive measures therefore implies a risk-taking for individuals who are not prepared to accept those. It is impossible for them not to maintain their social relations, while the daily life of the vast majority of individuals is marked by solidarity and reciprocity, without which people would find themselves in a difficult situation. The maintenance of these networks is therefore regarded of higher importance to the detriment of the prevention of the epidemic, which is perceived as an object of political manoeuvring. The transposition of international recommendations on epidemic management cannot ignore local contexts. Contradicting the initial view of the Covid-19 epidemic in Guinea, which perceived this disease as the pathology of the rich and the elite, the contamination is now generalised within the population of Conakry, regardless of social status and activity. The spread of the infection does not, however, invalidate the interest of a reflection linking social networks and Covid-19. Today, Guinean society must deal with the after-effects of Covid-19 (Brown et al., 2022) or long COVID (Leperre et al., 2020). This is reflected in new, temporary or permanent symptoms (Thallapureddy 11et al., 2022) , which individuals will have to manage in part by relying on their networks. It is therefore important in this context to understand what cognitive and material capacities will be available to them to manage unknown after-effects.
Acknowledgements
I would like to thank Professor Frédéric Le Marcis and Dr Sidy Cissokho for reading previous versions of this paper, as well as the reviewers, the translators and the Editorial Committee.